SCOPE: Care Groups
What is a Care Group?
Global evidence has shown the effect of the Care Group model on improving health outcomes. A Care Group (CG) is composed of 10-12 Care Group Volunteers (CGVs) who meet regularly for social behavior change communication (SBCC) and related skills-building on health education topics. After receiving the lessons, each CGV cascades information to 10-15 neighbor mothers in nearby households through group meetings and home visits.
In 1995, World Relief developed the CG model in Mozambique, and since then, the model has gained global recognition and received significant funding through USAID-funded programs worldwide. Due to the model’s effectiveness, nongovernmental organizations working in over 40 countries have implemented the CG model. A CG’s unique ability to extend the health system’s reach through the multiplication of volunteer effort, peer support, and community mobilization makes the model ideal for many projects and programs.
World Relief, through the USAID-funded SCOPE project, established CGs in Haiti, Kenya, Malawi, and South Sudan, equipping them to implement a SCOPE-developed series of training modules adapted from existing USAID-approved curricula. Promoter manuals and volunteer flipcharts included the latest evidence-based best practices on RMNCH information, each adapted for a particular country and its local communities. Each of the four modules was translated and underwent a contextualization process to ensure the messages, stories, and images were locally relevant. The CG model ensured that social behavior change health information was communicated using vernacular language and practiced through simple exercises performed at the household level.
During CG meetings, guided discussions were centered around clear learning objectives. To help facilitate discussions with neighbor women at home or during group meetings, each CGV was equipped with a pictorial flip chart to assist in presenting the lessons in a user-friendly and interactive way.
How Care Groups Impact Survival Outcomes

Extending the Reach of the Health System
CGs extended the reach of the health system down to the household level, ensuring that those who lived in hard-to-reach areas knew how and when to access health services. SCOPE CGVs complemented the work of overburdened community health workers (CHWs) by supporting case-finding and referrals so that CHWs could maximize their time in providing information and health services to the clients who needed them most. Through 18,910 CGVs, 192,355 women of reproductive age (WRA) were reached with information to improve RMNCH behavior and practices.
Providing a Key Source of Referrals
CGVs were a vital link between the community and facility services, in that they became a mechanism of the local referral system. Not only did CGVs provide information to their neighbor group members, but they could also recognize warning signs among pregnant women and children under five, and thus make the necessary referrals to the CHWs and facilities.
CGVs were trained to record and report on key vital events such as childbirth, pregnancy, child illnesses, and deaths, as well as provide timely referrals to CHWs who could feed information into existing health information systems. The Care Group model is particularly useful as it can reach a large population while maintaining cost-efficiency, sustainability, and intensive support to CGVs and beneficiaries.
This referral relationship also highlighted the difference between CHWs and CGVs. CHWs have a health background and training that CGVs do not, so the two should be viewed as an extension of each other rather than parallel entities. Therefore, careful consideration must be made regarding remuneration and incentivization. Many of these volunteers and health workers come from the same communities, and differences in incentives can be a source of conflict.
Care Group Structure
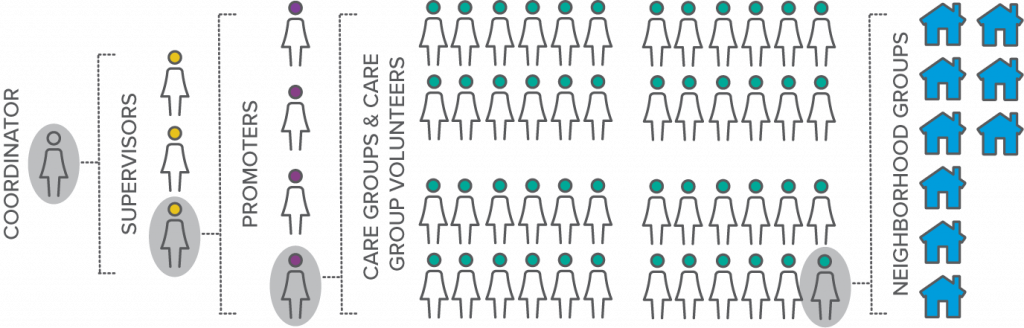
Coordinators (paid staff) are responsible for 3-6 Supervisors. Supervisors (paid staff) are responsible for 4-6 Promoters. Promoters support 4-9 CGs which are composed of 10-15 CGVs. CGVs share lessons with 10-15 Neighbor Groups (made up of Neighbor Women and their families). Through this cascade process each Promoter reaches approximately 500-1,200 women via CGVs.
Care Groups for Improved Family Planning and Maternal and Child Health Outcomes
Care Groups for Improved Family Planning and Maternal Child Health Outcomes
The system of group lesson delivery, home visits, and regular mentoring and supervision of CGs fostered peer-to-peer support, facilitated community-wide interest and improved health-seeking behavior among caregivers.
However, Care Groups were not only focused on diffusing messages, but also building their skills to reflect on what they have learned, issues they face, changing behavior, and solving problems together. As Rehema, a SCOPE Kenya CG Promoter in Kajiado reflected on the role of CGs in her community, “One transformed woman is the start point for the change to other women of this community.” In several project geographies, SCOPE found that the CG approach significantly facilitated positive behavior at scale within communities. Women took action in their households and communities. For example, it was observed that CGs across the SCOPE countries improved their hand-washing practices, built tippy taps and latrines using local resources, and grew vegetable gardens.
Despite the challenges from COVID-19 and region-specific political and environmental factors, Care Groups contributed to the positive results noted in the Midterm Evaluation. SCOPE teams reported stories of community members turning their knowledge into action, and rallying around women and young children to advocate for their healthcare needs at local facilities.
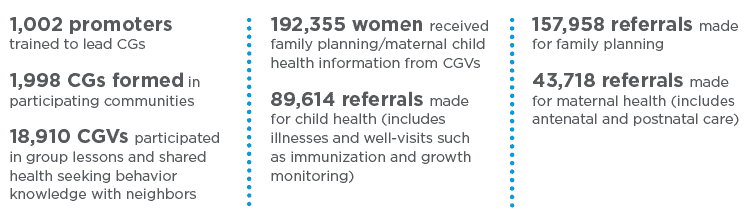
Key Results
Teams reported stories of community members turning their knowledge to action. Below is a snapshot of the project’s results of the Care Group model across the SCOPE countries:
Hear the stories of transformation through SCOPE Care Groups














